
Conditions
Mr Kosuge offers specialist assessment and treatment for the full range of hip and knee conditions listed below. He sees patients privately at The Rivers Hospital, Sawbridgeworth, and on the NHS at The Princess Alexandra Hospital, Harlow. Patients travel from across West Essex and East Hertfordshire — including Bishop's Stortford, Epping, Hertford, Chelmsford, and Ware — to receive specialist orthopaedic care.
For each condition, Mr Kosuge begins with a thorough assessment and explores all appropriate non-surgical options before considering surgery. Where surgery is required, he uses evidence-based techniques and provides detailed pre- and post-operative support throughout your care.
GENERAL

-
An inflammatory arthritis that predominantly affects the spine, Ankylosing spondylitis (AS) can also lead to fatigue and eye problems. Other joints may also be affected by pain and swelling.
-
Arthritis is a broad term describing conditions that cause pain, inflammation, and stiffness in one or more joints. It is one of the most common reasons people seek orthopaedic advice, and affects people of all ages — though it becomes more prevalent with age.
The most common forms relevant to hip and knee surgery are osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis following previous injury or fracture. Gout and other crystal arthropathies may also affect the hip and knee joints. Mr Kosuge is experienced in assessing and managing all forms of arthritis affecting the hip and knee, and will tailor his approach to your specific diagnosis, symptom pattern, and lifestyle. Treatment ranges from non-surgical measures to joint replacement, depending on the extent and impact of your condition.
-
The smooth surfaces of the bones in the knee joint are covered by a specialised tissue called hyaline cartilage, which allows painless, low-friction movement. When this cartilage is damaged — whether through injury, repetitive stress, or underlying disease — pain, swelling, and mechanical symptoms such as locking or catching can result.
A chondral injury refers to damage confined to the cartilage layer, whilst an osteochondral injury involves both the cartilage and the underlying bone. These injuries can occur in isolation, particularly in younger, active patients, or as part of a broader arthritic process. Mr Kosuge assesses cartilage injuries using clinical examination and MRI imaging, and can discuss the full range of treatment options — from physiotherapy and injections through to surgical procedures including arthroscopy, microfracture, or cartilage restoration techniques.
-
Gout is a form of inflammatory arthritis caused by the deposition of uric acid crystals within joints and surrounding tissues. It characteristically presents as sudden, severe attacks of pain, swelling, warmth, and redness — most commonly affecting the joint at the base of the big toe, though the ankle, knee, and other joints may also be involved.
Whilst gout is primarily managed with medication to control uric acid levels, the knee can be significantly affected during acute flares and in cases of chronic tophaceous gout. Mr Kosuge can assess knee pain in the context of a possible gout diagnosis, arrange appropriate investigations, and advise on management. In rare cases where gout has led to significant joint damage, surgical options may be considered.
-
Joint hypermobility describes an increased range of movement in one or more joints beyond what is considered normal. It is more commonly seen in younger patients and women, and in many people is entirely asymptomatic — and may even be an advantage in activities such as dance, gymnastics, or music.
However, a significant minority of people with hypermobility experience joint pain, instability, recurrent soft tissue injuries, and fatigue — a presentation sometimes referred to as hypermobility spectrum disorder or hypermobile Ehlers-Danlos Syndrome (hEDS). The hip and knee joints are commonly affected, and patients may experience pain, a sensation of joints giving way, or difficulty with activities such as prolonged standing or walking. Mr Kosuge can assess hip and knee symptoms in the context of hypermobility, and will work alongside physiotherapy and other specialists as appropriate to develop a management plan tailored to your needs.
-
Lower back pain is one of the most common conditions in the UK and is a frequent reason for GP and specialist consultations. In the vast majority of cases it is benign and self-limiting, though it can be significantly disabling when severe or recurrent.
An important reason why lower back pain features on this page is that it can closely mimic hip pain — and vice versa. Pain arising from the lumbar spine can radiate into the buttock, groin, and thigh, making it difficult to distinguish from true hip pathology without careful clinical assessment. Mr Kosuge is experienced in differentiating between spinal and hip sources of pain. When the history and examination suggest that pain is arising from the hip joint, further investigation and treatment can be offered. Where pain appears to be primarily spinal in origin, Mr Kosuge will direct you to the most appropriate specialist. A hip injection performed under image guidance can be a useful diagnostic tool in cases where the source of pain is unclear.
Patient Information Leaflet from Mr Kosuge →
British Association of Spine Surgeons →
-
Osteoarthritis (OA) is the most common form of arthritis and the leading cause of musculoskeletal disability in the United Kingdom. It involves the gradual breakdown of the articular cartilage that lines the surfaces of joints, accompanied by changes to the underlying bone, joint lining, and surrounding soft tissues. Whilst it is commonly described as 'wear and tear', this is an oversimplification — the condition involves active biological processes affecting the entire joint rather than simply the passive wearing away of cartilage.
Osteoarthritis most commonly affects the knee, hip, hands, and spine. Risk factors include increasing age, previous joint injury, obesity, and genetic predisposition. Symptoms develop gradually and include pain, stiffness (particularly after rest), swelling, and reduced range of movement. Mr Kosuge specialises in the assessment and management of hip and knee osteoarthritis, offering the full spectrum of treatments from conservative management and injections through to joint replacement surgery. He sees patients from across Essex and Hertfordshire at his clinics in Sawbridgeworth and Harlow.
-
Rheumatoid arthritis (RA) is a chronic systemic autoimmune condition in which the body's immune system mistakenly attacks the lining of the joints (the synovium), causing inflammation, pain, swelling, and over time, damage to cartilage and bone. It is the second most common form of arthritis and can affect multiple joints throughout the body, including the hips and knees.
Significant advances in disease-modifying anti-rheumatic drugs (DMARDs) and biologic therapies over recent decades have dramatically reduced the proportion of patients with RA who require surgery. However, when joint damage is severe and quality of life is significantly affected despite optimal medical treatment, joint replacement surgery remains an important and effective option. Mr Kosuge works alongside rheumatologists and can assess patients with RA who have significant hip or knee involvement, advising on whether and when surgical intervention may be appropriate.
HIP
-
Avascular necrosis (AVN) — also known as osteonecrosis — of the femoral head is a condition in which the blood supply to the ball of the hip joint is disrupted, leading to the death of bone tissue. Without an adequate blood supply, the bone gradually collapses, causing progressive pain and, if untreated, severe destruction of the hip joint.
AVN can be associated with prolonged or high-dose corticosteroid use, excessive alcohol consumption, trauma to the hip, blood clotting disorders, sickle cell disease, and certain other medical conditions. In some cases, no identifiable cause is found. Early-stage AVN may be managed with procedures such as core decompression to restore blood flow, whilst more advanced cases often require hip replacement surgery. Mr Kosuge is experienced in both the assessment and surgical management of AVN and will advise on the most appropriate treatment based on the stage of the disease and your individual circumstances.
-
Developmental dysplasia of the hip (DDH) describes a spectrum of conditions in which the ball and socket of the hip joint have not developed normally. The socket (acetabulum) may be too shallow or maloriented, the ball (femoral head) may be positioned abnormally, or the joint may be frankly dislocated. DDH is typically identified in infancy or childhood through screening programmes, though milder forms may not become apparent until adolescence or adulthood.
When DDH is not adequately treated in childhood, the abnormal mechanics of the hip joint place excessive stress on the cartilage, leading to early-onset osteoarthritis — often presenting in patients in their thirties or forties. Mr Kosuge can assess adult patients with known or suspected DDH, including those presenting with hip pain at a younger age than is typical for osteoarthritis. Treatment options depend on the degree of dysplasia and the extent of any arthritic change, and may range from activity modification and physiotherapy to hip replacement surgery in those with advanced joint damage.
-
A groin strain describes an injury to the muscles or tendons of the groin region, most commonly involving the adductor muscle group on the inner aspect of the thigh. These injuries are particularly common in sports that involve rapid changes of direction, kicking, or sprinting — such as football, rugby, and hockey — but can also occur following a fall or awkward movement.
Symptoms typically include pain in the inner thigh or groin, aggravated by bringing the legs together or raising the knee. Severity ranges from mild discomfort to complete muscle or tendon tears. It is important to distinguish a groin strain from other causes of groin pain, including hip joint pathology, labral tears, hernias, and nerve-related conditions, as the management of each differs significantly. Mr Kosuge can assess groin pain comprehensively and will arrange appropriate investigations — such as MRI — to reach an accurate diagnosis and guide treatment.
-
The hamstrings are a group of three muscles — the biceps femoris, semitendinosus, and semimembranosus — that run along the back of the thigh from the sitting bone (ischial tuberosity) of the pelvis to just below the knee. They play a vital role in bending the knee and extending the hip, and are among the most commonly injured muscles in sport.
Hamstring injuries range from mild strains involving a small number of muscle fibres through to complete tears, and may occur anywhere along the muscle or at its attachments. High-grade tears at the proximal (upper) attachment — at or near the ischial tuberosity — can be particularly disabling and may require surgical repair if conservative treatment fails. Mr Kosuge can assess the full spectrum of hamstring injuries, arrange appropriate imaging, and advise on the optimal management pathway, including whether surgical intervention is likely to be of benefit.
Patient Information Leaflet from Mr Kosuge →
-
The acetabular labrum is a ring of fibrocartilage that lines the rim of the hip socket, deepening the joint and providing stability, as well as helping to maintain a protective fluid seal within the hip. A labral tear — a disruption in this structure — is an increasingly recognised cause of hip pain, particularly in younger and more active patients.
Labral tears most commonly occur in association with underlying structural abnormalities of the hip, such as femoroacetabular impingement (FAI) — where abnormal bony prominences cause the ball and socket to pinch against each other — or hip dysplasia. Less commonly, tears arise from acute trauma or repetitive high-intensity activity. Symptoms typically include pain deep in the groin, often described as a catching or clicking sensation, and may be worsened by prolonged sitting, pivoting, or high-impact activities. MRI arthrography is the investigation of choice. Management depends on the severity of the tear and the underlying cause, and may include physiotherapy, injections, or hip arthroscopy in selected cases.
-
Meralgia paraesthetica is a condition caused by irritation or compression of the lateral femoral cutaneous nerve — a purely sensory nerve that supplies sensation to the outer (lateral) aspect of the thigh. Patients typically describe burning, tingling, numbness, or aching pain over the outer thigh, which may worsen with prolonged standing or walking and improve when sitting.
Common causes include compression of the nerve as it passes under the inguinal ligament near the hip, which may be related to obesity, pregnancy, tight clothing, or a large belt. In some cases, scar tissue following previous surgery or a hip replacement can be responsible. The condition is usually managed conservatively with activity modification, weight management if appropriate, and in some cases, local anaesthetic or steroid injection around the nerve. Surgery to decompress or divide the nerve is occasionally considered in refractory cases. Mr Kosuge can assess outer thigh pain and distinguish meralgia paraesthetica from other causes of hip and thigh discomfort.
-
Osteoarthritis of the hip is the most common reason for hip replacement surgery in the United Kingdom. The condition involves the gradual loss of the smooth articular cartilage covering the ball and socket of the hip joint, leading to bone-on-bone contact, pain, stiffness, and progressive loss of function. Bony spurs (osteophytes) often develop around the joint margins as the body attempts to compensate for the loss of cartilage.
Hip osteoarthritis typically presents in patients over the age of fifty, though it can affect younger people — particularly those with underlying conditions such as hip dysplasia or previous hip injury. Symptoms include groin pain that is typically worse with activity and improves with rest in the early stages, morning stiffness, a reduced range of movement, and in more advanced cases, pain at rest or at night. Mr Kosuge offers the full range of treatment for hip osteoarthritis — from non-surgical management including physiotherapy, weight management advice, and hip injections, through to total hip replacement when conservative measures are no longer sufficient. A dedicated page on hip osteoarthritis is available on this website. He sees patients from across Essex and Hertfordshire at The Rivers Hospital, Sawbridgeworth, and The Princess Alexandra Hospital, Harlow.
Mr Kosuge’s Webpage on Hip Osteoarthritis →
Patient Information Leaflet from Mr Kosuge →
American Academy of Orthopaedic Surgeons →
American Academy of Orthopaedic Surgeons (Animation Video) →
-
Snapping hip syndrome — also known by the Latin term coxa saltans — describes an audible or palpable snapping sensation arising from the hip during movement. It is a common complaint, particularly in young and physically active individuals, and can be felt at the front, side, or within the hip joint itself, depending on the underlying cause.
The three principal causes are: (1) the iliotibial band snapping over the greater trochanter on the outer hip; (2) the iliopsoas tendon flicking over the front of the hip joint; and (3) intra-articular pathology such as a loose body or labral tear causing catching within the joint itself. The first two causes are often painless and may require no treatment beyond reassurance and physiotherapy. The third — intra-articular snapping — is more likely to be associated with pain and may warrant further investigation with MRI. Mr Kosuge can accurately identify the cause of snapping hip symptoms and advise on the most appropriate management, which may range from physiotherapy and activity modification to injection or, in selected cases, surgical treatment.
-
Greater trochanteric pain syndrome (GTPS) — previously and more narrowly termed trochanteric bursitis — describes pain over the outer aspect of the hip, centred on the bony prominence of the greater trochanter. It is one of the most common causes of hip-region pain and is particularly prevalent in middle-aged women, though it can affect people of all ages and backgrounds.
The condition involves inflammation or degeneration of the tendons of the gluteal muscles where they attach to the greater trochanter, often in association with bursitis (inflammation of the fluid-filled sacs overlying the bone). Symptoms include localised tenderness over the outer hip, pain that is often worse when lying on the affected side, climbing stairs, or standing on one leg. GTPS is frequently misdiagnosed as hip joint arthritis, and careful clinical assessment is important to distinguish between the two. Treatment is predominantly non-surgical, including physiotherapy with specific tendon-loading exercises, activity modification, and corticosteroid injection. In cases that fail to respond to conservative management, further options including platelet-rich plasma (PRP) injection may be considered.
Patient Information Leaflet from Mr Kosuge →

KNEE

-
Iliotibial band (ITB) syndrome is one of the most common causes of outer knee pain in endurance athletes, particularly runners, cyclists, and rowers. The iliotibial band is a thick band of connective tissue that runs along the outer aspect of the thigh from the hip to just below the knee. In ITB syndrome, the band becomes irritated as it repeatedly moves over the lateral femoral epicondyle — the bony prominence on the outer side of the knee — during repetitive flexion and extension.
Symptoms typically include a sharp or burning pain on the outer side of the knee, which comes on at a predictable point during exercise and may force the patient to stop activity entirely. The pain usually settles quickly with rest but recurs with the next session. Risk factors include training errors (particularly sudden increases in mileage), leg length discrepancy, and hip abductor weakness. Management centres on physiotherapy with a structured rehabilitation programme, biomechanical assessment, and temporary activity modification. Corticosteroid injection may be considered in cases that fail to respond to physiotherapy alone.
-
The menisci are two C-shaped wedges of fibrocartilage — the medial meniscus on the inner side and the lateral meniscus on the outer side — that sit between the thighbone (femur) and shinbone (tibia) in the knee joint. They act as shock absorbers, improve joint stability, and distribute load across the knee. A meniscal tear is one of the most common knee injuries, occurring both in active individuals following twisting injuries and in older patients as a result of degenerative change.
Symptoms of a meniscal tear may include pain along the inner or outer joint line of the knee, swelling, stiffness, and in some cases, locking or a sensation of the knee giving way. Not all meniscal tears require surgery — many, particularly those associated with underlying osteoarthritis, are best managed with physiotherapy and non-surgical measures. Mr Kosuge will assess your symptoms and imaging carefully and advise on the most appropriate management, which may include physiotherapy, injection, arthroscopic meniscal trimming (partial meniscectomy), or in suitable cases, meniscal repair.
Patient Information Leaflet from Mr Kosuge →
-
The knee is the joint most frequently affected by osteoarthritis, making it the leading indication for knee replacement surgery in the United Kingdom. The condition involves the progressive loss of articular cartilage on the surfaces of the femur, tibia, and patella within the knee, accompanied by changes to the underlying bone and joint lining. As cartilage is lost, the joint space narrows and the bones begin to contact each other, causing pain, inflammation, and reduced function.
Symptoms develop gradually and include pain that is typically worse with activity — particularly going up and down stairs or rising from a chair — morning stiffness, swelling, a grinding or creaking sensation (crepitus), and in more advanced cases, deformity of the knee and pain at rest or at night. Mr Kosuge offers the full spectrum of treatment for knee osteoarthritis, beginning with non-surgical options including physiotherapy, weight management, and injections (steroid, hyaluronic acid, PRP, and Arthrosamid), through to surgery including partial and total knee replacement. A dedicated page on knee osteoarthritis is available on this website. He consults at The Rivers Hospital, Sawbridgeworth, and The Princess Alexandra Hospital, Harlow.
Mr Kosuge’s Webpage on Knee Osteoarthritis →
-
An osteochondral injury is a focal area of damage to the articular cartilage of the knee joint and the bone immediately beneath it. Unlike the generalised cartilage loss seen in osteoarthritis, osteochondral injuries tend to be localised defects that may arise following an acute injury, repetitive stress loading, or as a result of osteochondritis dissecans — a condition in which a segment of bone and its overlying cartilage loses its blood supply and may separate from the surrounding bone.
Symptoms can include pain (often localised to a specific area of the knee), swelling, stiffness, and mechanical symptoms such as locking or catching if a fragment has become loose within the joint. MRI is the investigation of choice for characterising osteochondral lesions. Treatment depends on the size, location, and stability of the lesion, as well as patient age and activity level, and ranges from conservative management and physiotherapy through to arthroscopic procedures including debridement, microfracture, and cartilage restoration techniques. Mr Kosuge will discuss all appropriate options with you.
-
Patellar tendinopathy — commonly known as 'jumper's knee' — is a painful condition affecting the patellar tendon, which connects the lower pole of the kneecap (patella) to the upper shinbone (tibial tubercle). It is most common in athletes who participate in jumping and explosive sports such as basketball, volleyball, and athletics, though it can also affect non-athletes following a sudden increase in physical activity.
The condition involves degeneration of the tendon at a cellular level, often at its attachment to the lower patella, and is characterised by localised tenderness at this point, together with pain during and after loading activities — particularly jumping, squatting, or going down stairs. A key feature is that pain often improves during activity but worsens again afterwards. Management is primarily non-surgical and centres on a structured physiotherapy programme incorporating progressive tendon-loading exercises (eccentric and heavy slow resistance training). In cases that fail to respond, options including injections (corticosteroid, PRP) or extracorporeal shockwave therapy may be considered.
-
Patellofemoral pain syndrome (PFPS) is one of the most common causes of knee pain, particularly in young and physically active individuals. It arises from dysfunction in the way the kneecap (patella) tracks over the lower end of the thighbone (femur) during movement, resulting in abnormal pressure on the cartilage of the patellofemoral joint.
Symptoms typically include a diffuse, aching pain at the front of the knee or around the kneecap, which is aggravated by activities that load the patellofemoral joint — such as going up or down stairs, squatting, prolonged sitting with the knee bent (sometimes called the 'cinema sign'), and running. The condition is more prevalent in women and may be associated with factors including hip muscle weakness, altered lower limb biomechanics, foot pronation, and training errors. Treatment is non-surgical in the vast majority of cases and focuses on physiotherapy with targeted strengthening of the hip abductors and quadriceps, correction of any underlying biomechanical factors, and activity modification. Mr Kosuge can assess and confirm the diagnosis, excluding other structural causes of anterior knee pain where appropriate.
Patient Information Leaflet from Mr Kosuge →
-
Pes anserine bursitis is an inflammation of the bursa located at the inner (medial) aspect of the knee, just below the joint line. The pes anserinus — Latin for 'goose's foot', describing the fan-like arrangement of three tendons (sartorius, gracilis, and semitendinosus) that attach in this region — overlies a small fluid-filled sac (bursa) that can become inflamed and painful.
The condition is most commonly seen in overweight or obese patients with knee osteoarthritis, and in runners. Symptoms include pain, tenderness, and sometimes swelling on the inner side of the knee, typically below the joint line — a location that helps to distinguish it from medial collateral ligament injury or medial compartment arthritis. Pain is often worse at night and on climbing stairs. Management typically involves physiotherapy, activity modification, weight management where relevant, and in many cases a corticosteroid injection into the bursa, which can be highly effective. Mr Kosuge can assess inner knee pain and arrange imaging if needed to confirm the diagnosis.
-
Pre-patellar bursitis — colloquially known as 'housemaid's knee' — is inflammation of the bursa that lies directly in front of the kneecap (patella), between the skin and the bone. This small fluid-filled sac normally allows smooth movement of the skin over the patella, but when irritated or inflamed it can become significantly swollen and tender.
The most common cause is repeated or prolonged kneeling — hence the traditional name — and it is therefore an occupational hazard for those in trades such as carpet fitting, plumbing, and gardening. It may also occur following a direct blow to the front of the knee, or as a result of infection (septic bursitis) or inflammatory conditions such as gout or rheumatoid arthritis. The pre-patellar swelling is typically well-defined and sits directly over the kneecap rather than within the joint itself, helping to distinguish it from a joint effusion. Non-infective cases are usually managed conservatively with rest, compression, and anti-inflammatory medication. Where infection is suspected, urgent aspiration and antibiotics are required. Surgical drainage or removal of the bursa (bursectomy) is occasionally needed for recurrent or refractory cases.
Patient Information Leaflet from Mr Kosuge →
Treatments
HIP
-
Before considering any surgical procedure, Mr Kosuge will always explore the full range of non-surgical treatment options with you. For many patients, non-operative management provides significant and sustained relief and may avoid or delay the need for surgery.
Non-operative treatments for hip pain include: analgesic and anti-inflammatory medication to manage pain and reduce inflammation; a structured physiotherapy programme focused on strengthening the muscles supporting the hip, improving flexibility, and optimising movement patterns; hydrotherapy (water-based exercise), which is particularly beneficial for patients with significant pain or limited mobility on land; and weight management, as reducing body weight significantly decreases the load on the hip joint and can lead to meaningful improvements in pain and function. Activity modification — adjusting the type, intensity, or duration of physical activity — is also an important component of conservative management. Mr Kosuge will discuss all relevant options and work with you to develop a plan that is tailored to your lifestyle, preferences, and treatment goals.
Chartered Society of Physiotherapy →
-
A hip joint injection involves the introduction of medication — typically a corticosteroid combined with a local anaesthetic — directly into the hip joint. It is performed under image guidance (fluoroscopy or ultrasound) to ensure accurate placement, usually as an outpatient or day-case procedure.
Hip injections serve two important purposes. As a diagnostic tool, they are particularly valuable in cases where it is unclear whether pain is arising from the hip joint itself or from an adjacent structure such as the lumbar spine — if a hip injection provides significant temporary relief, this strongly suggests the hip is the primary source of pain and may support the case for hip replacement. As a therapeutic tool, injections can provide meaningful pain relief, allowing patients to engage more effectively with physiotherapy and improving quality of life, particularly when surgery is being deferred. The duration of benefit varies between patients. Mr Kosuge will advise you on whether a hip injection is appropriate in your particular circumstances and arrange the procedure at The Rivers Hospital, Sawbridgeworth.
-
Core decompression is a surgical procedure used in the treatment of avascular necrosis (AVN) of the femoral head, typically in the earlier stages of the disease before significant collapse of the femoral head has occurred. The procedure involves drilling one or more channels through the outer cortex of the femur into the area of affected bone, with the aim of reducing the elevated intra-osseous pressure that contributes to ongoing ischaemia, and stimulating a healing response by encouraging blood vessel ingrowth.
Core decompression can be performed as a standalone procedure or augmented with bone grafting, stem cell or growth factor preparations, or other biological adjuncts to further promote healing and bone regeneration. The procedure is performed under general or spinal anaesthesia and is typically a day-case or short-stay operation. Recovery involves a period of protected weight-bearing to allow healing. Whilst core decompression is most effective in early-stage AVN, it is not always successful in preventing disease progression, and some patients will ultimately require hip replacement surgery. Mr Kosuge will assess the stage of your AVN carefully using MRI imaging before advising on whether core decompression is likely to be of benefit in your case.
-
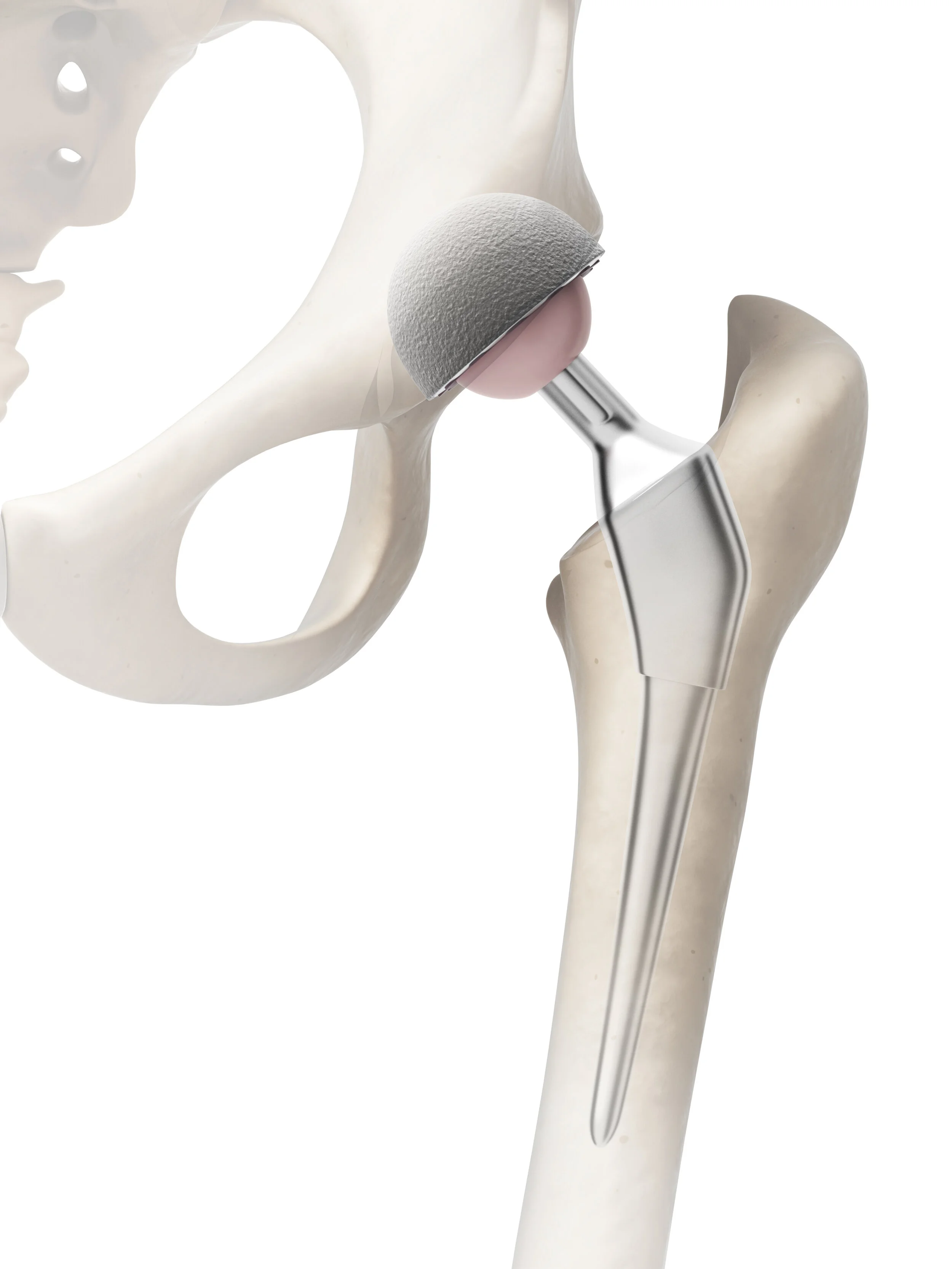
Total hip replacement (also called total hip arthroplasty) is one of the most successful and commonly performed operations in all of surgery. It involves removing the damaged ball and socket of the hip joint and replacing them with a prosthetic implant, restoring smooth, pain-free movement. The procedure has an excellent track record, with the large majority of patients experiencing a dramatic improvement in pain and function that is sustained over many years.
Mr Kosuge performs hip replacements at The Rivers Hospital, Sawbridgeworth, for private patients, and at The Princess Alexandra Hospital, Harlow, for NHS patients. Full information about hip replacement — including what to expect from the procedure, recovery, and Mr Kosuge's outcomes data — is available on the dedicated hip replacement page of this website. If you are considering a hip replacement, Mr Kosuge warmly invites you to book a consultation to discuss your options.
Mr Kosuge’s Webpage on Hip Replacement →
Patient Information Booklet from Mr Kosuge →
Versus Arthritis patient information booklet →
American Academy of Orthopaedic Surgeons (Animation Video) →
International Cartilage Regeneration & Joint Preservation Society (Animation Video) →
-
Revision hip replacement is the surgical removal and replacement of a previously implanted hip prosthesis that has failed or is no longer functioning adequately. It is a technically more demanding procedure than primary hip replacement, requiring the removal of existing implants that may be well-fixed to bone, the management of any associated bone loss, and the insertion of new components that can achieve reliable fixation in a compromised environment.
Mr Kosuge has developed particular expertise in revision hip replacement surgery, including the management of complex acetabular (socket) defects, and was co-author of an award-winning presentation on surgical reconstruction of severe acetabular defects at the American Academy of Orthopaedic Surgeons (AAOS) in 2019. A dedicated page on revision hip replacement is available on this website. If you are experiencing problems with a previous hip replacement, Mr Kosuge offers specialist assessment at The Rivers Hospital, Sawbridgeworth, and The Princess Alexandra Hospital, Harlow.
Mr Kosuge’s Webpage on Revision Hip Replacement →
Patient Information Leaflet from Mr Kosuge →
American Academy of Orthopaedic Surgeons →
American Association of Hip and Knee Surgeons (Patient Guide) →
International Cartilage Regeneration & Joint Preservation Society (Animation Video) →
KNEE

-
Non-surgical treatment is the appropriate first step for the majority of patients presenting with knee pain, and for many patients it provides sufficient and lasting relief. Mr Kosuge will always explore conservative options fully before discussing surgical alternatives.
Non-operative treatments for knee pain include: analgesic and anti-inflammatory medication; a structured physiotherapy programme to strengthen the quadriceps, hamstrings, and hip muscles that support the knee, improve joint stability, and address any underlying biomechanical factors; hydrotherapy for patients who find land-based exercise too painful; and weight management, as even modest weight loss can have a meaningful impact on pain and function in patients with knee arthritis. Activity modification and the use of appropriate footwear or orthotic insoles may also be beneficial. For patients with knee osteoarthritis who have not responded adequately to these measures, knee injections (see below) offer a further non-surgical option before surgery is considered
Chartered Society of Physiotherapy →
-
Knee injections are a non-surgical treatment option for knee pain, most commonly used in the management of osteoarthritis. Several different agents can be injected, each with a different mechanism of action, and the evidence base for each varies. Mr Kosuge will discuss all options with you and advise on which, if any, is most likely to be of benefit in your particular situation.
Corticosteroid (steroid) injection is the most established option, acting to reduce joint inflammation and providing pain relief that typically lasts weeks to several months. Hyaluronic acid (viscosupplementation) is injected to supplement the natural joint fluid and may provide a longer duration of relief in some patients, though the evidence is more variable. Platelet-rich plasma (PRP) uses a concentration of the patient's own blood platelets — which contain growth factors — injected into the joint to promote a healing and anti-inflammatory response. Arthrosamid is a novel hydrogel injection that cushions the joint and may provide durable pain relief. Mr Kosuge will advise on the most appropriate option based on your diagnosis, symptom pattern, and individual circumstances.
Steroid:
Hyaluronic acid:
American Academy of Orthopaedic Surgeons →
International Cartilage Regeneration & Joint Preservation Society →
Platelet-Rich Plasma:
American Academy of Orthopaedic Surgeons →
International Cartilage Regeneration & Joint Preservation Society →
Arthrosamid:
-
Knee arthroscopy is a minimally invasive ('keyhole') surgical procedure in which a small camera (arthroscope) and fine surgical instruments are introduced into the knee joint through small incisions, allowing the surgeon to visualise and treat a range of conditions from within the joint. It is typically performed under general as a day-case procedure, requiring no overnight stay in most cases.
Arthroscopy allows Mr Kosuge to treat conditions including meniscal tears (trimming or repair), cartilage damage, removal of loose bodies, and some cases of synovial inflammation. It is important to note that the role of arthroscopy in the management of knee osteoarthritis is limited and often not recommended. Mr Kosuge will explain clearly whether arthroscopy is likely to be of benefit in your case, and will provide detailed written information about the procedure, preparation, what to expect on the day, and how to manage your recovery. Full information is available in his dedicated Patient Information Booklet on Knee Arthroscopy
Patient Information Booklet from Mr Kosuge →
American Academy of Orthopaedic Surgeons →
Royal College of Anaesthetists →
International Cartilage Regeneration & Joint Preservation Society (Animation Video) →
-
Partial meniscectomy — the arthroscopic trimming of a torn meniscus — is one of the most commonly performed knee operations. It involves the removal of the unstable, torn portion of the meniscus using fine instruments introduced through small keyhole incisions, whilst preserving as much healthy meniscal tissue as possible.
It is the most frequently used surgical treatment for a symptomatic meniscal tear, and is generally most appropriate when the tear is in the inner (avascular) zone of the meniscus — where blood supply is limited and healing is unlikely — or where the tear pattern is not amenable to repair. The procedure is typically performed as a day case under general anaesthesia, with most patients able to bear weight and return to light activities within a few days. Return to sport or more demanding activities will take longer. It is important to note that meniscal trimming is not appropriate in all cases, and Mr Kosuge will assess whether this procedure is the right option for you based on your symptoms, MRI findings, and the characteristics of the tear.
Patient Information Booklet from Mr Kosuge →
International Cartilage Regeneration & Joint Preservation Society (Animation video) →
-
Meniscal repair is the arthroscopic procedure in which a torn meniscus is stitched back together rather than trimmed away. The goal is to preserve the meniscal tissue and restore its normal function — an important consideration given the meniscus's vital role in load distribution, shock absorption, and joint stability. Preserving the meniscus also helps to protect the knee from the earlier development of osteoarthritis that can follow meniscal loss.
However, meniscal repair is not appropriate for all types of tear. It is most likely to succeed in tears that occur in the outer (vascular) zone of the meniscus, where blood supply is sufficient to support healing, and in younger, active patients with an otherwise healthy joint. Recovery following meniscal repair is longer than after trimming, as a period of protected weight-bearing and restricted range of movement is required to allow the repair to heal — typically up to 3 months. Mr Kosuge will assess the characteristics of your tear carefully and discuss whether repair is a viable and preferable option compared with partial meniscectomy in your specific case.
Patient Information Booklet from Mr Kosuge →
International Cartilage Regeneration & Joint Preservation Society (Animation video) →
-
Microfracture is an arthroscopic surgical technique used to treat focal cartilage defects in the knee. The procedure involves making multiple small perforations (microfractures) through the calcified layer at the base of a cartilage defect and into the underlying bone marrow. This releases bone marrow stem cells and growth factors into the defect, stimulating the formation of a fibrocartilaginous repair tissue that partially restores the joint surface.
Whilst fibrocartilage is not identical to the native hyaline cartilage it replaces — it is less durable and may deteriorate over time — microfracture can provide meaningful pain relief and functional improvement, particularly in younger patients with smaller, well-defined defects on weight-bearing surfaces. Post-operative rehabilitation requires a period of protected weight-bearing to allow the repair tissue to form and mature. Microfracture is generally considered most appropriate for defects under two square centimetres in younger patients with good surrounding cartilage and minimal underlying arthritis. Mr Kosuge will advise on whether microfracture is an appropriate option for your cartilage defect, and will discuss alternative cartilage restoration techniques where relevant.
Royal Orthopaedic Hospital NHS Foundation Trust →
International Cartilage Regeneration & Joint Preservation Society (Animation video) →
-
Partial knee replacement — also known as unicompartmental knee replacement (UKR) — is a surgical procedure in which only the arthritic compartment of the knee is resurfaced and replaced, while the unaffected compartments and the cruciate ligaments are preserved. It is an excellent option for appropriately selected patients, offering the benefits of a more natural-feeling knee, a smaller incision, less bone and tissue disruption, a shorter hospital stay, and a faster recovery compared with total knee replacement.
Patient selection is critical to achieving a good outcome. Partial knee replacement is most suitable for patients with osteoarthritis confined to one compartment of the knee — most commonly the medial (inner) compartment — with intact cruciate ligaments and a correctable deformity. Mr Kosuge will assess your suitability carefully, reviewing your symptoms, examination findings, and with appropriate investigations. A dedicated page on partial knee replacement, including full details of the procedure and recovery, is available on this website. Mr Kosuge performs partial knee replacements at The Rivers Hospital, Sawbridgeworth.
Mr Kosuge’s Webpage on Partial Knee Replacement →
Patient Information Booklet from Mr Kosuge →
-
Total knee replacement (also known as total knee arthroplasty) is a highly effective surgical procedure for patients with advanced knee arthritis that is significantly impacting quality of life despite adequate non-surgical management. The procedure involves removing the damaged bone and cartilage from the ends of the femur (thighbone), tibia (shinbone), and in most cases the back of the patella (kneecap), and replacing them with precision-engineered metal and plastic components that recreate a smooth, functioning joint surface.
Total knee replacement consistently delivers substantial improvements in pain, mobility, and quality of life, and is one of the most cost-effective procedures in all of medicine. Mr Kosuge performs total knee replacements, including robotic-assisted total knee replacements, at The Rivers Hospital, Sawbridgeworth. A dedicated page on total knee replacement with full information about the procedure and recovery is available on this website. Private and NHS appointments are available at Sawbridgeworth and The Princess Alexandra Hospital, Harlow, respectively.
Mr Kosuge’s Webpage on Total Knee Replacement →
Patient Information Booklet from Mr Kosuge →
Mr Kosuge’s Webpage on Robotic-Assisted Total Knee Replacement →
Versus Arthritis Patient information booklet →
American Academy of Orthopaedic Surgeons (Animation Video) →